


 Sign Out
Sign Out
Premedication: PAXUS PM therapy does not require premedication to prevent hypersensitivity reactions. However, premedication may be given approximately 30 minutes prior to PAXUS PM administration, depending on the judgment of physicians in order to minimize the possibility of severe hypersensitivity reactions. Such premedication may consist of hydrocortisone 100 mg IV (or its equivalent), pheniramine maleate 45.5 mg IV (or its equivalent), and cimetidine 300 mg or ranitidine 300 mg or ranitidine 50 mg IV (or its equivalent).
Dose Adjustment: Dose can be reduced to Level-2 based upon the degree of toxicities experienced by patients who receive PAXUS PM therapy. If patients are not tolerant at a reduced dose of Level-2, discontinuation of this drug should be considered. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFirst dose adjustment (240 mg/m2): For patients who experience febrile neutropenia or who experience severe neutropenia (<500 cells/mm3) or thrombocytopenia (<50,000 cells/mm3) for more than one week, dose reduction to Level-1 should be considered. For patients with Grade 3 neurological toxicities, dose reduction to the Level-1 should be considered. For patients with Grade 4 neurological toxicities, discontinuation of this drug should be considered.
Second dose adjustment (190 mg/m2): If patients experience the recurrence of above toxicities after administration of Level-1 dose, additional dose reduction should be made to Level-2. For Grade 3/4 non-hematologic toxicities (except nausea, vomiting, and alopecia), the administration of this drug should be held till the recovery for up to 3 weeks, otherwise dose reduction or discontinuation of this drug should be considered. For Grade 1 or more increase/decrease in body weight, dosage may be recalculated based upon body surface and adjusted in the range of ±5 mg of recalculated dose.
After discontinuation of this drug due to hypersensitivity reactions, the therapy can be resumed by the judgment of physician. At resumption, patients should receive premedication and the same dosage of PAXUS PM as the previous therapy before discontinuation (the reduced dose in case of a dose reduction due to toxicities). When this resumption shows a tolerable result, premedication can be given afterwards.
Non-small Cell Lung Cancer: PAXUS PM is administered by intravenous infusion over 3 hours according to the following dose instructions, followed by cisplatin 60 mg/m2 intravenous infusion every 3 weeks.
Premedication: All patients should be premedicated approximately 30 minutes prior to PAXUS PM administration in order to prevent severe hypersensitivity reactions. Such premedication may consist of hydrocortisone 100 mg IV (or its equivalent), pheniramine maleate 45.5 mg IV (or its equivalent), and cimetidine 300 mg or ranitidine 50 mg IV (or its equivalent). Ondansetron 8 mg IV (or its equivalent) may be administered as prophylactic anti-emetics prior to cisplatin administration.
Dose Adjustment: The recommended initial dose of PAXUS PM is 230 mg/m2. Dose adjustment for the subsequent courses PAXUS PM should be decided with consideration of dose increase/reduction conditions according to the following table. For patients with toxicities corresponding to dose reduction conditions, dose should be reduced to the Level -1, and -2. For patients who are not tolerant to the lowest dose level (Level-2, 145 mg/m2), discontinuation of this drug should be considered. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDose can be increased when all of the following conditions are fulfilled after the first administration of drug: In hematological analysis at the first and second week of the first cycle, absolute neutrophil count = 1.0 x 109/L and thrombocyte count = 100 x 109/L.
In hematological analysis prior to subsequent cycles of PAXUS PM, recovery of hematogenetic function, absolute neutrophil count = 1.0 x 109/L and thrombocyte count 100 x 109/L .
Dose can be increased in Grade 2 or lower non-hematological toxicities, but should be maintained in Grade 2 non-hematological toxicities related to this drug (in Grade 1, 2 or 3 nausea, vomiting, alopecia, myalgia and arthralgia, dose can be increased).
Dose should be reduced when one of the following conditions is observed after each cycle: In febrile neutropenia, severe neutropenia (<500 cells/mm3) or thrombocytopenia (<50,000 cells/mm3) more than one week, dose should be reduced to a lower dose level.
In Grade 2 neurological toxicities, dose should be reduced to a lower level. In Grade 3 or higher neurological toxicities, discontinuation of therapy should be considered.
In Grade 2 hepatic toxicities related abnormal bilirubin or ALP, SGOT, and SGPT, dose should be reduced to a lower dose level, in Grade 3 hepatic toxicities related abnormal bilirubin or ALP, SGOT, and SGPT elevations and discontinuation of therapy should be considered.
In order non-hematological toxicities, dose should be reduced to a lower dose level at Grade 2 and discontinuation of therapy should be considered at Grade 4 (except nausea, vomiting, alopecia, myalgia, and arthralgia). Once dose is reduced due to toxicities, the dose should not be increased (except the recovery of liver function).
Preparation of Solution for Infusion: Preparation of Pre-Mix Solution (Paclitaxel 6 mg/mL): PAXUS PM should be reconstituted by injection 5 ml of 0.9% Sodium Chloride Injection to each vial of PAXUS PM with aseptic syringe and a needle and swirling gently to dissolve.
The reconstituted solution is a colorless to bluish solution. If foaming are visible due to a solubilizing ingredient of drug, it is recommended to wait the disappearance of foaming up to 5 minutes and use it at once, but not required to wait until the complete disappearance of forming.
Preparation of Solution for Infusion: The reconstituted solution should be taken with a calibrated syringe and diluted with 0.9% Sodium Chloride Injection or 5% Dextrose injection to a final concentration of 0.6-3.0 mg/mL and swirled gently for complete mixing. It should be inspected visually prior to administration. If particular matters are observed, discard the solution.
The physical and chemical stability of the solution for infusion is as follows; See Table 3.
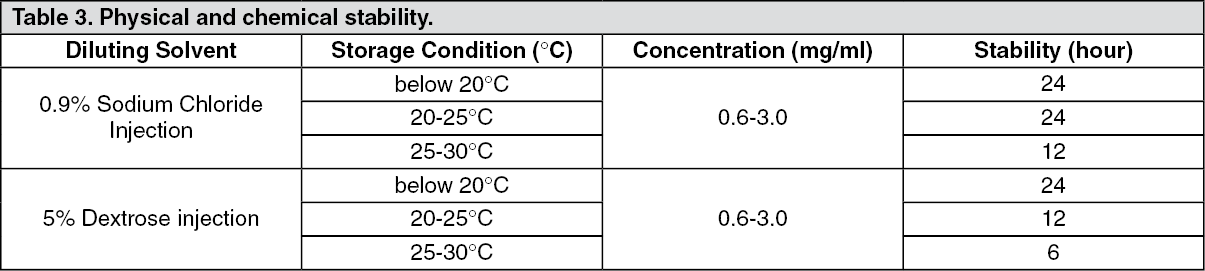 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image